Warning – This post containes graphic pictures !
Cognitive – Behavioral Therapy – (CBT)
Aleksandra Rataj and Dagna Skrzypinska from CBT center in Cracow talked a bit about the terapautic methods that can be used to help women with MRKH.

CBT is based on the theory that learning affects people’s behavior, thoughts and feelings.
It is a way of talking about how humans:
- Look at themselves, the world and other people
- How do the things you do affect one’s thoughts and feelings

The psychological impact on women with MRKH syndrome:
Studies on individual cases and small – medium sized cases seen in retrospect says:
- Adapting to MRKH syndrome is a difficult and traumatic process
- Unsure of her female identity
- Experiencing a form of insecurity / confusion about their gender, body, social and sexual role
- Greater risk of develop a negative view of themselves
- Many women look at themselves as defective, inferior or unlovable
- Surgical or dilator treatment are often experienced as shameful may serve to perpetuate or strengthen these beliefs
- Although the successful creation of a neovagina ameliorates remove some of these difficulties MRKH has a lasting effect, perpetuating these women’s negative view on themselves.
Psychological distress:
- MRKH women had significantly higher scores on depression and anxiety
- Women with MRKH had significantly higher scores on the items confidence than other women with MRKH.
- No difference in women with or without MRKH with interpersonal relationships
- Eating Disorders – Women with MRKH had a significantly higher score in terms of eating disorders. In contrast to the comparison with women without MRKH, the women with MRKH had a higher score negatively on self-awareness, trust in other people, ineffectiveness and Bulimia.
CBT group intervention
- Aim: to address the three key factors that maintains an unhelpful adjustment to MRKH
- The Intervention centered on a CBT case with conceptualization which guides the therapy.
- As therapy progresses, each woman produced her own conceptualization tailored to her circumstances.
- Each session addresses a different MRKH related topic.
- The women were taught to identify unhelpful coping strategies and to replace them with more adaptive techniques.
- Finally, there was an attempt to help women find meaning in their experience.
- In the session the different strengths and perspectives of group members were used to brainstorm new ways of dealing with MRKH syndrome.
- Between sessions, the women were instructed to write down their thoughts in homework. In addition to tasks related to the topics raised in the group, and specially designed exercises to promote better emotional adjustment to past issues that women have avoided to talk about. And to teach women a better technique that will give them a better balance in their view of themselves.
- At the end of the sessions, women were asked to write down a «goodbye» letter as a reflection of what they had learned.
Result:
- The women in the group / program showed significant reduction in psychological symptoms, and an insignificant change in all the other points at the end of the sessions and by monitoring their treatment. Those on the waiting list showed no signs of change in any direction.
- The conclusion is therefore that women receiving CBT treatment improves their psychological health by MRKH.
Next woman out was Philomeena Weijenborg, Gynecologist from the Netherlands with 30 years of experience with women affected by MRKH at Leiden University. She has had about 300 patients with MRKH.

She talked about the effect of having a group program for women with MRKH. They have also done studies where they have looked at the women’s reactions in relation to:
- Medical History – What was done how it was informed to them that they have MRKH and how was their first reaction.
- Reaction of family, parents, friends and partner. Then and now?
- Do you have a vagina, how did you decide treatment and were you informed of all the methods that can be used.
- Sexuality, then and now
- Infertility – How do you cope?
- female role and femininity
In the Netherlands dilation method is the first choice, and they avoid surgery if possible.
They have established that MRKH can cause mental stress on the girls.
It depends entirely clear that the group program where girls with MRKH get to meet each other have a very positive effect on girls.
They have once a year a national gathering for girls with MRKH and a day were parents, partners, friends and siblings can join.
The home page of their org is http://www.stichtingmrk.nl
They are also working to identify the sexual function in women and the factors that influence. It is mentioned among other things:
- Stress and sexual function
- Sexual function before diagnosis
- Traumatic experiences / sexual abuse
- Partner sexual experience, compared
- Nonwestern cultures and religions
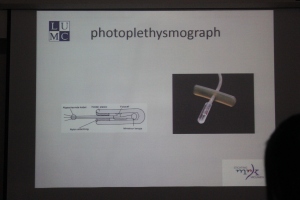
- What neovagina is best?
In the future they will also study the physiological sexual arousal response in surgical and non surgical created neovaginas of women with MRKH.
They insert the devise into the vagina while the woman is getting relaxed in a chair and an erotic film is being shown. The device will then be able to gauge how excited the women are.

They would like to point out from their experiences that:
- MRKH is not a disease!
- Support groups are unique and very valuable
- Frank’s method (dilation) is the preferred method for creating a vagina.
- Guidelines based on facts for health professionals and gynecologists are sorely needed.
Philomeena was a great woman, easy to talk to and showed a tremendous support and care for us. There were several girls who got teary eyed of being greeted with such care. She was really amazing!
Verena Henninger works at Tübingen Universistes hospital in Germany.

She was incredibly calm and she also had a tremendous care for her patients and MRKH women.
At Tubingen, they have a separate MRKH center where they treat girls. They get such a good follow-up after the diagnosis and follow-up after treatment.
Here they have strong focus on giving the patient good and correct information, have their own support groups and days where women can meet each other and specialists.
Their diagnostic procedure is the following:
- History
- Ultrasound
- Digital Palpation – vaginally or rectally
- Chromosome analysis
- Hormonal status
- (diag.LSC)
Treatment:
Non surgical:
- Dilation – Frank’s method
Benefits:
- No risk of problems arising from the operation
- No scars
Disadvantages:
- Pain Fully
- Long time to achieve the desired result may be difficult to implement for a long time.
- Neovaginal prolapses due to lack of friction
- Risk of dilation in the urethra
Operations:
The transplant:
- Leather (McIndoe)
- Intestine (sigma, ileum, rectum)
- Peritoneum (Davydov)
Without a transplant:
- Minimal harmful surgical method
Surgical treatments:
Bowel neovagina
Disadvantages:
- Fetid discharge
- Colitis
- Serious complications ex Anastomosis,
- Large Technical Operation
- Prolapse of the vagina
- Cancer
Benefits:
- As a rule, no danger that the vagina shrinks in retrospect
- No problems with getting wet
- No dilation after the operation.
Peritoneum + Leather transplant neovagina
Disadvantages:
- Shrinks – Dilation rest of the life
- No lubrication / difficult to get wet
- Fake vagina walls / not natural vaginal walls
- Prolapse / collapsing – your vagina can colapse
- Shorter length of vagina
- Hair can grow on the inside because the skin is transplanted
- scarring
Benefits:
- Short hospital stay
- No special instruments are needed later.
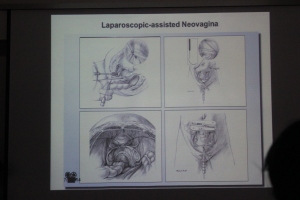
Laparoscopic assisted neovagina:
This is the method they use at Tübingen. The women receive good support both before and after surgery. They inserts a Tractive apparatus and within 3-4 days the vagina is 10 cm deep.
Here’s more details on how it is done:


Treatment after the operation:
- Peridural Catheters – removed when the traction device is removed
- Urethral Catheter – Removed when traction device removed
- Antibiotics – until traction device removed
- Postoperative dummy – (estrogen cream)
- Dummy used for 12 weeks 24 hours in a day, the next 12 weeks use 10 hours every third night. (only at night)
- intercourse possible after 4 weeks.
Patients are followed up from 11 to 141 months after the operation, depending on the progress of the patient.
Average length of vagina after such an operation is 9.5 cm.
On average dummy is used in 8.5 months.
Conclusion:
- Creates a vagina that is of normal depth, and functions well
- Safe and non-traumatic method
- Long-term satisfactory results
This method is their first choice in the treatment of their patients. They also accepts patients from other countries.
Psychological support:
- The assistant psychologist is there in the time before and during surgery and or combined with follow-up sessions at the clinic.
- Support for family and partner interviewed
- Customized questions for patients to follow their evolution / adaptation
Based on their experience, the average patient with MRKH has no more troubled mentally / psychologically than other women of the same age.
Saturday, November 29, 2014 they will have their fourth MRKH meeting at their clinic Tübingen.
The following topics are planned at the meeting:
- Interaction with other MRKH women
- Presentation of the latest research
- Information about MRKH and Treatment
- Information on adoption
- Psychological consultation
- Partner discussions
Website: http://www.neovagina.de
Karina Kapczuk Polish PhD , working with MRKH patients. She told us about their administrasion of MRKH syndrome.

The focus is on:
- How to create a neovagina
- Rudimentary uterine horns and pelvic pain
- Hypersensitivity
The method used is Wharton vagina plastic



20 of 36 patients who had surgery between 1995 and 2009 were followed up from 2007 to 2010
Result:
- Vaginas length ranged from 4.5 to 12 cm with an average of 6.3 cm.
- The completely satisfaction measured on a scale where 6 is the maximum satisfaction showed these 18 patients:
- 2 were not sexually active
- Lust score 3.6
- Arousal 4.5
- Lubrication / wetness 5.7
- Orgasm 4.2
- Satisfaction 5.6
- Pain 4.8
Total score 28.2
There was no association between the vagina’s dimensions and the total score.
Rudimentary Uterine Horn and Pelvic pain:

- Clinical manifestations – excessive hair growth
- Etiology – Polisystisk ovary syndrome
Treatment:
- Antiandrogen (used in monotherapy)
- Cyproterone medicine
- Spironolactone
- Finasteride
- Oral contraceptives (continued use after treatment)
Karina Sasin presented her survey done in Poland on Polish women with MRKH to show how these experiences where based on their own expectations. 40 patients participated in the study

Diagnosis:
- Average age of diagnosis ring was 17 years (ranged from 12 to 22)
- 6 patients (15%) were adequately examined at the first consultation with the doctor
- 12 (30%) received complete information
- 20 (50%) received some information
- 8 (20%) received no information
- 13 (33%) had no support from family or friends
- 17 women (43%) felt rejected
- 33 patients (83%) felt that they where experimental rabbits
Treatment:
- 33 (83%) were treated
- 22 underwent vaginal plastic surgery Average age was 19.4 with a rank of 12 to 25 years.
- 14 Veechietti
- 4 modified Wharton
- 2 Krzeski (leather from the bladder)
- 1 Bowel – unspecified
- 11 dilation treatments – mean age 19.9
- Sexual satisfaction: 2 out of 10 for those who completed surgery and 1 of 10 in the dilation group
- 23 (58%) willing to undergo a womb transplant
Recommendations and practices:
- USA – Frank’s method (dilation) as the first treatment, if this does not work they recommend surgery where one does not take skin from your body. However, the practice varies widely.
- UK – Recommend Frank’s method
- SWEDEN – No national recommendations, Vecchietti vaginoplasty
- RUSSIA – RAMS / MoH recommends Davydov
To read the survey in its entirety you can find the original one here

Tilbaketråkk: Oppsummering MRKH møte Polen 3-6 Juli Del 2 | mrkhnorge
Tilbaketråkk: 2014 in Review – English Version – mrkhnorge